Physical Causes
Most ED in men over 40 has a physical component. The big ones:
Cardiovascular disease and high blood pressure
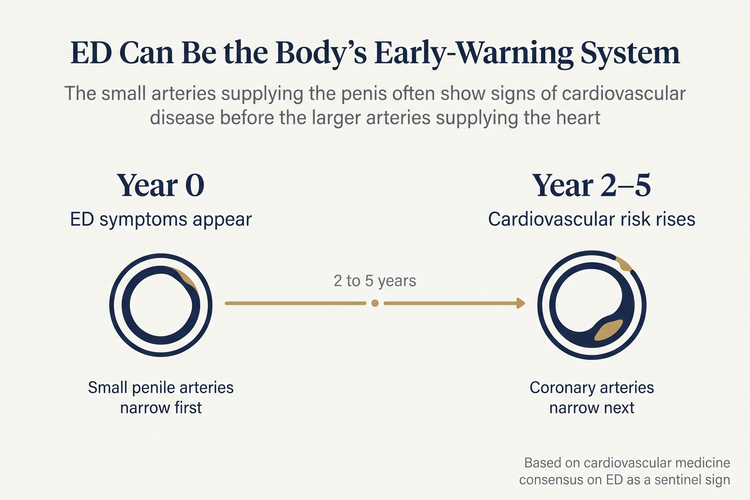
Erections are a vascular event — they need healthy blood flow. Anything that narrows or stiffens the small arteries (high blood pressure, high cholesterol, atherosclerosis) reduces the blood supply needed for a firm erection. Because the penile arteries are smaller than the coronary arteries, ED can show up as a warning sign before a heart attack or stroke.
Diabetes
Diabetes — particularly when blood sugar is poorly controlled over years — damages both the small blood vessels and the nerves involved in erection. ED in men with diabetes tends to start earlier, occur more often, and respond less well to oral medications such as PDE5 inhibitors than in non-diabetic men — though these medications remain effective first-line treatment, and outcomes improve substantially when blood sugar control is addressed alongside. Good diabetes control reduces the risk of ED and improves how well treatment works.
Hormonal causes
Low testosterone can contribute to reduced libido (interest), reduced morning erections, and sometimes ED itself. It's not always the main driver, but it's worth ruling in or out — particularly if there are other low-testosterone symptoms like fatigue, mood changes, or loss of muscle mass. A simple morning blood test is the starting point.
Less commonly, thyroid dysfunction (both an overactive and underactive thyroid) can affect erectile function, and a raised prolactin level (sometimes due to a small benign pituitary issue) can cause low libido and ED. Both are picked up on simple blood tests when there's a clinical reason to check.
Prostate cancer treatment
ED is one of the most common after-effects of prostate cancer treatment. Surgery (radical prostatectomy), radiotherapy, and certain hormone therapies all affect erectile function — sometimes temporarily, but often long-term. Even with modern nerve-sparing surgery and refined radiotherapy planning, long-term outcomes remain significant: at 10 years post-treatment, around 60–80% of men report erections insufficient for intercourse. If you've had any of these treatments and developed ED, a tailored discussion with your doctor about post-treatment options is worthwhile.
Nerve damage and neurological conditions
Spinal cord injury, multiple sclerosis, Parkinson's disease, stroke, and nerve damage from bladder surgery or pelvic trauma can all cause ED. So can long-standing diabetes (through nerve damage).
Anatomical and other physical factors
Conditions like Peyronie's disease (scarring inside the penis causing curvature), low blood flow from venous leak, and chronic kidney or liver disease can all contribute.